
Medial vs Lateral Meniscus: Symptoms, Treatment & Recovery
The knee is a complex joint, and few injuries are as common or as widely misunderstood as a meniscus tear. When patients hear “torn cartilage,” they are often referring to the meniscus. However, not all meniscus tears are created equal. Meniscal tears tend to be classified as degenerate, where even turning over in bed can lead to a tear or acute non-degenerative, which often involve the knee twisting in a slightly flexed position and are often associated with ligament injuries.
When deciding on management, the location of the tear, its chronicity (degenerate vs. non-degenerate) and associated ligament or cartilage pathology determine how a meniscus is treated. Understanding the meniscus anatomy can help to explain how and why certain tears are treated with surgery, why some are repaired and others partially removed and why some are managed without surgery at all. This guide aims to clarify the rationale behind the treatment of meniscus injury.
Understanding the Meniscus Anatomy
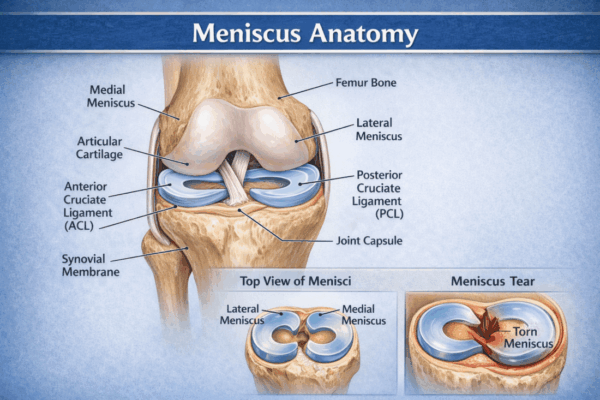
Your knee has two C-shaped pieces of tough, rubbery cartilage that act as shock absorbers between your shinbone (tibia) and thighbone (femur). These are your menisci. Their primary purpose is to distribute load, stabilise the knee joint, and provide lubrication for smooth movement. Without them, the articular cartilage covering the ends of the bones would wear down quickly, leading to arthritis.
Key Differences Between Medial and Lateral Menisci
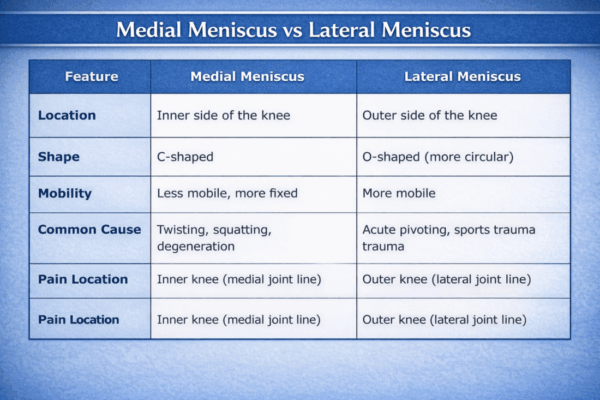
Structurally, the medial and lateral menisci differ in ways that influence how and why they get injured. The medial meniscus, on the inner side of the knee, is more C-shaped and is firmly attached to the tibia, joint capsule and the medial collateral ligament (MCL). This rigid attachment makes it less mobile and, therefore, more susceptible to tearing. It bears up to 50% of the load on the inner compartment of the knee.
In contrast, the lateral meniscus, on the outer side of the knee, is more circular or o-shaped and has more mobility. It covers a greater area of the tibial cartilage and is not as firmly fixed to the surrounding structures, allowing it to move back and forth during knee flexion and extension. This mobility helps it accommodate the rotational forces of the knee, but it is not immune to injury. It handles approximately 70% of the load on the outer compartment. Lateral meniscus tears tend to happen in the context of ligament injuries, such as an ACL rupture. They are also more likely to heal due to a robust blood supply.
Meniscal Zones and Their Healing Potential
The menisci are divided into three zones each. The periphery or outer part of the meniscus is called the ‘red zone’. It receives the best blood supply from its attachments to the joint capsule and other surrounding structures. ‘Red zone’ tears have the best healing potential of all meniscal tears.
The inner part is called the ‘white zone’. This area has a very poor blood supply and thus has the least healing potential. The ‘white zone’ relies on the surrounding joint fluid for its nutrition. White zone tears, which cause mechanical symptoms such as a clicking, catching or locking sensation with twisting, are often treated by meniscectomy or removal of the offending meniscus tissue.
The zone in between, called the ‘red-white’ or ‘pink zone’, has a relatively decent blood supply and, in certain tear morphologies, is amenable to repair. It does not heal as well as the red zone, but it is much better at healing than the white zone tears.
In addition, there are 2 anchor points at the front and back of the tibia where the menisci are attached. These anchors are crucial structures to the meniscus function. When an anchor is lost, the meniscus loses tension, and the knee behaves as if there is no meniscus at all. Meniscus root or anchor tears are almost always treated with surgery unless you have significant arthritis in the joint.
Symptoms of Meniscus Tears
While there is some overlap, the symptoms can often point toward which meniscus is injured. Listening to your body and noting the precise location of the pain are crucial first steps.
Medial Meniscus Symptoms
A medial meniscus tear typically presents with pain located specifically on the inner side of the knee.
- Inner-knee pain: Pain concentrated along the medial joint line.
- Pain when squatting: Deep knee flexion compresses the torn fragment, causing sharp pain.
- Joint line tenderness: The area over the inner knee joint will be tender to the touch.
- Clicking or catching: A sensation that something is getting caught inside the joint during movement.
Lateral Meniscus Symptoms
Pain from a lateral meniscus tear is felt on the outer side of the knee.
- Outer-knee pain: Sharp pain along the lateral joint line is a hallmark symptom.
- Swelling: Lateral tears are often associated with more significant and rapid swelling (effusion) compared to degenerative medial tears.
- “Shift” or “give way” sensation: A feeling of instability, as if the knee might buckle.
- Pain with twisting: Pivoting on the affected leg will often elicit sharp, localised pain.
What Causes Meniscus Tears?
Meniscus tears fall into two main categories: acute (traumatic) and degenerative.
- Athletic Twisting Injuries: This is the classic cause of a meniscus tear, especially in younger individuals. A sudden pivot, cut, or twist while the foot is planted firmly on the ground can create a shearing force that tears the cartilage. This is common in sports like soccer, basketball, and skiing. These forces can cause both a medial and a lateral meniscus tear.
- Degenerative Wear: In adults over 40, the meniscus can lose its elasticity and become more brittle. In these cases, a tear can occur with minimal trauma, such as rising from a chair or stepping awkwardly. These degenerative tears are more common in the medial meniscus. A meniscus root tear, a specific and severe type of degenerative tear, can also occur.
- Sudden Pivoting or Deep Squatting: Activities that involve deep, forceful knee bending or rotation can trap and tear the meniscus.
- Repetitive Kneeling: Certain occupations that require prolonged kneeling can place chronic stress on the menisci, leading to fraying and eventual tearing.
Diagnosis
An accurate diagnosis is the cornerstone of effective treatment. While symptoms provide clues, a definitive diagnosis requires a clinical evaluation and often advanced imaging.
- Physical Examination: A specialist will perform a series of physical tests to stress the menisci. The McMurray test and Thessaly test involve bending, straightening, and rotating the knee to see if these movements reproduce the pain or a clicking sensation, indicating a probable tear. The location of the joint line tenderness (medial vs lateral) is also a strong indicator.
- MRI as Gold Standard: Magnetic Resonance Imaging (MRI) is the best way to visualise the soft tissues of the knee. It can confirm the presence of a meniscus tear, identify its location and pattern (e.g., meniscus root tear), and rule out or identify other associated injuries, like ligament damage or cartilage defects. Early imaging is crucial for planning the right course of treatment.
For a comprehensive overview of meniscus injuries, see our Meniscus Injury Guide.
Treatment Options
Treatment for a meniscus tear depends on the type, size, and location of the tear, your age, activity level, and symptoms. Options range from conservative management to advanced surgical intervention.
Non-Surgical Treatment
For small tears or degenerative tears without significant mechanical symptoms, a conservative approach is often the first line of management.
- RICE Principles: Rest, Ice, Compression, and Elevation can help manage initial pain and swelling.
- Physiotherapy: A targeted physiotherapy program is crucial. It focuses on strengthening the quadriceps and hamstrings to better support and stabilise the knee joint, thereby reducing the load on the meniscus. With a multi-disciplinary, multi-modal rehabilitation program, certain meniscal tears can be managed successfully without surgery. Dr Cohen uses trusted physiotherapists who offer tailored, modern approaches to help rehabilitate patients with meniscal tears at both his Kogarah and Bondi Junction practices.
Surgical Options
When non-surgical treatment fails or for larger, unstable tears causing mechanical symptoms, surgery may be recommended. This is almost always performed arthroscopically (keyhole surgery).
- Arthroscopic Meniscus Repair: Whenever possible, repairing the torn meniscus is preferred. The surgeon stitches the torn pieces back together, preserving the knee’s natural shock absorber. This is most successful for tears in the “red zone” or outer part of the meniscus, which has a blood supply conducive to healing.
- Partial Meniscectomy (Debridement): If the tear is in a region with poor blood supply (the “white zone”) or the tissue is of poor quality, the damaged portion of the meniscus is trimmed away. The goal is to remove the unstable fragment causing pain while preserving as much healthy tissue as possible. Up to 30% of meniscal tissue can be removed without significantly impacting the knee or leading to rapidly progressive arthritis.
- Meniscus Root Repair: A tear at the “root” where the meniscus attaches to the bone is a serious injury. Repairing this is critical to restoring joint function and preventing rapid-onset arthritis.
- Meniscus Transplant: In rare cases, for young patients who have previously had most of their meniscus removed and are experiencing pain, a transplant using donor tissue may be considered.
Explore our Knee Pain page for more information on potential causes and treatments.
Recovery Timeline
Recovery depends entirely on the treatment performed. Following your surgeon’s protocol is essential for a successful outcome.
Recovery After Non-Surgical Treatment
With physiotherapy and activity modification, symptoms from minor tears can improve significantly in 2–6 weeks.
Recovery After Partial Meniscectomy
Recovery is much faster because no tissue healing is required.
- Walking: Often possible on the same day as surgery.
- Return to Office Work: Within 1 week.
Return to Sport: Generally 4–6 weeks
Recovery After Meniscus Repair
This is a longer process, as the repaired tissue needs time to heal.
- Brace and Protected Weight-Bearing: Typically required for up to 6 weeks.
- Return to Running: Around 3-4 months.
- Return to Sport: Usually between 4–6 months, depending on healing and strength.
When to See a Knee Specialist
You should consult an orthopaedic specialist if you experience:
- Persistent knee pain that does not improve with rest.
- Mechanical symptoms like catching, locking, or giving way.
- Significant or recurrent swelling.
- Inability to pivot, twist, or squat without pain.
An experienced knee surgeon in Bondi Junction and Kogarah with a special interest in meniscus injuries can provide an accurate diagnosis and a tailored treatment plan. Early intervention often leads to better long-term outcomes and helps preserve the health of your knee joint.
Book a Consultation
If you’re experiencing knee pain or possible meniscus symptoms, an accurate diagnosis is the most important step. Dr Dan Cohen consults in Bondi Junction and Kogarah, treating a full range of knee injuries from meniscus tears to complex ligament reconstructions.
Book a consultation today or view our clinic locations to take the first step toward recovery.